Feasibility and Competency Outcomes of a Standardized Colonoscopy Curriculum in General Surgery Residency
Article information

Abstract
Background
Integrating structured colonoscopy training into general surgery residency programs remains both a logistical and educational challenge. This study evaluated the feasibility and educational outcomes of a standardized colonoscopy training curriculum for surgical residents using objective competency assessments and trainee perceptions.
Methods
A retrospective mixed-methods analysis was conducted among general surgery residents who participated in a standardized colonoscopy training program between 2022 and 2025. Faculty assessed objective procedural competency using the Direct Observation of Procedural Skills framework across three domains: basic manipulation, anatomical understanding, and insertion & advancement. Trainee perceptions regarding the training environment, procedural difficulty, and perceived educational value were evaluated using a post-training survey.
Results
Objective competency data from 369 residents were analyzed. Residents demonstrated high performance in the basic manipulation and anatomical understanding domains following completion of the training program. In contrast, scores in the insertion & advancement domain were comparatively lower, suggesting greater technical difficulty. Post-graduate year (PGY)-3 residents achieved significantly higher scores than PGY-2 residents in this domain (p=0.015), whereas performance in the other domains was comparable between the groups. Post-training survey responses indicated that most residents considered the training duration and group size appropriate, and more than 94% reported that the program would be beneficial for their future clinical practice.
Conclusions
A standardized colonoscopy training curriculum implemented during surgical residency was feasible and was associated with high levels of competency in fundamental endoscopic skills. However, insertion and advancement techniques remained more challenging for junior trainees, suggesting that additional practice opportunities targeting complex insertion skills may improve future training programs.
Introduction
Proficiency in colonoscopy is an essential skill for general surgeons, as it plays a central role in colorectal cancer screening, diagnostic evaluation, and perioperative management of colorectal diseases. High-quality colonoscopy has been associated with improved adenoma detection and reduced colorectal cancer incidence and mortality, highlighting the importance of adequate training and procedural competence [1-3].
Traditionally, endoscopic training in surgical residency has followed an apprenticeship-based model in which trainees acquire procedural skills through supervised clinical exposure. Although experiential learning remains fundamental to procedural education, reliance on opportunistic case exposure can result in substantial variability in training experiences depending on institutional case volume, instructor availability, and local educational practices [4,5]. In recent years, medical education has increasingly adopted competency-based training frameworks that emphasize clearly defined learning objectives, structured educational interventions, and objective assessment of procedural competence [6-8].
In the field of gastrointestinal endoscopy, several professional societies have emphasized the importance of structured training programs and competency-based assessment to ensure consistent procedural quality and patient safety [9,10]. Within such frameworks, objective evaluation tools—such as structured workplace-based assessments—have been introduced to evaluate technical performance in a standardized manner and support competency-based progression in procedural training [11,12].
Despite these developments, the optimal timing for introducing colonoscopy training during surgical residency remains a subject of discussion. While early exposure to procedural training may facilitate progressive skill acquisition, limited data are available regarding the specific technical challenges encountered by residents at different stages of training. Previous studies examining colonoscopy learning curves have shown that different procedural components develop at different rates, with tasks such as scope manipulation and anatomical recognition often acquired earlier, whereas loop management and advancement through complex colonic segments may require more extensive clinical experience [13-15].
Understanding these domain-specific learning patterns is important for designing effective training curricula. In addition to objective competency assessment, trainee perceptions of the educational environment and perceived procedural difficulty can provide valuable insights into educational needs and program feasibility [16,17].
Therefore, the aim of this study was to evaluate the educational outcomes of a standardized colonoscopy training program for general surgery residents using both objective competency assessment and trainee perceptions. Specifically, this study sought to (1) analyze domain-specific procedural competency using a structured Direct Observation of Procedural Skills (DOPS)-based assessment, (2) compare competency outcomes between residents undergoing training at different stages of residency, and (3) evaluate trainee perceptions regarding the educational environment and perceived value of the training program.
Materials and Methods
Study design and participants
This retrospective mixed-methods study evaluated the educational outcomes of a standardized colonoscopy training program for general surgery residents. The study included residents who participated in the program between 2022 and 2025. Participants were categorized into two cohorts according to the timing of the training: a traditional cohort (training conducted in 2022, targeting post-graduate year [PGY]-3 residents; n=145) and an early-intervention cohort (training conducted between 2023 and 2025, targeting PGY-2 residents; n=225). Because the dataset was fully anonymized, two residents who completed the training during their PGY-3 year in the early-intervention period could not be individually identified and were therefore retained in the 2023–2025 cohort for analysis.
The study protocol was approved by the Institutional Review Board (IRB) of Asan Medical Center, Seoul, Korea (IRB No. 2026-0291).
Standardized educational intervention
The standardized colonoscopy training program was designed using a flipped-learning model to maximize the efficiency of the hands-on training session (Fig. 1). Prior to attending the practical session, all residents were required to complete a video-based pre-learning module consisting of short instructional videos (approximately 5 minutes each). The modules covered four core topics: endoscopic system setup, basic insertion techniques, recognition of endoscopic anatomy, and documentation of key findings.
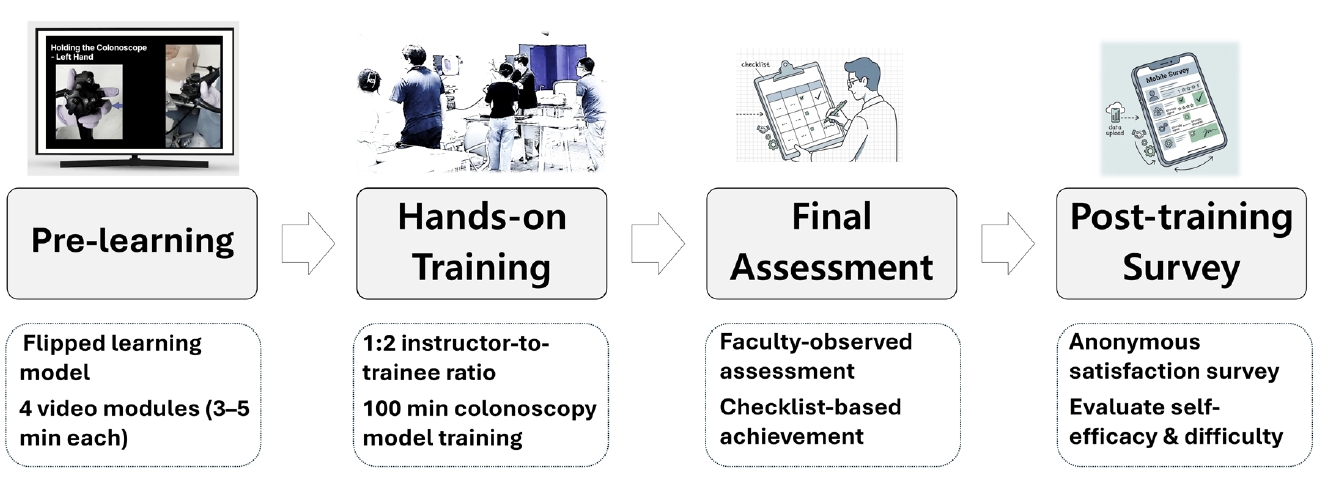
Structure of the standardized endoscopy training program. Schematic illustration of the training curriculum, which consisted of four sequential components: pre-learning, hands-on training, final competency assessment, and a post-training survey.
After completing the pre-learning module, residents participated in a structured half-day hands-on training session. Because the theoretical components were addressed during the pre-learning phase, the practical session focused entirely on procedural skill training under direct faculty supervision. The hands-on curriculum consisted of two dedicated training modules: 100 minutes of upper gastrointestinal endoscopy training and 100 minutes of colonoscopy training, allowing residents to practice fundamental scope manipulation, insertion techniques, and loop-reduction strategies in a supervised environment.
To ensure standardized instruction, training was conducted in small groups of six to seven residents supervised by three or four experienced instructors, maintaining an instructor-to-trainee ratio of approximately 1:2. This program was implemented as part of a standardized national training initiative for general surgery residents in Korea, supported by the Korean Surgical Society and the Korean Surgical Skill Study Group. Tutors were recommended by residency-training hospitals as faculty tutors with substantial colonoscopy experience and were selected from those who had participated in at least one tutor workshop held three times annually. The hands-on training was performed primarily using the Olympus EVIS EXERA III 290 system (Olympus), and colonoscopy simulation training was conducted using a Kyoto Kagaku colon simulator (Kyoto Kagaku Co., Ltd.). This structure allowed individualized feedback and sufficient procedural practice for each trainee.
Objective assessment (Direct Observation of Procedural Skills)
At the end of the training session, residents underwent a faculty-observed performance assessment. Procedural competency was evaluated using a structured checklist based on the DOPS framework and aligned with the program’s official evaluation rubric.
The checklist was designed to reflect the sequential workflow of colonoscopy and to evaluate both technical manipulation and anatomical recognition skills. The checklist consisted of 10 task-specific items reflecting the procedural workflow of colonoscopy, including scope manipulation, anatomical recognition, and safe advancement to the cecum (Table 1). The items were grouped into three competency domains: Basic Manipulation Skills (four items), Anatomical Understanding and Documentation (two items), Insertion and Advancement Skills (four items). To improve reproducibility, the core technical components of the standardized colonoscopy training program and the corresponding DOPS-based assessment framework are summarized in Supplementary Table 1.
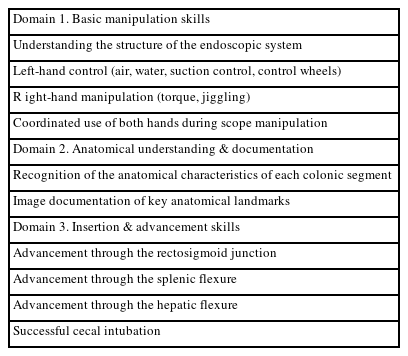
Assessment checklist for colonoscopy skills
Each item was rated by faculty using a 3-point scale (Excellent, Satisfactory, or Needs Improvement). For quantitative analysis, ratings were converted to numerical scores (Excellent=3 points, Satisfactory=2 points, Needs Improvement=1 point). Scores were summed within each domain to generate domain-specific performance scores. The maximum possible scores were 12 points for Basic Manipulation Skills, 6 points for Anatomical Understanding and Documentation, and 12 points for Insertion and Advancement Skills.
One resident in the 2023–2025 cohort was excluded because of missing evaluation data, resulting in a final sample of 369 residents for the objective analysis.
Subjective assessment (survey)
Following completion of the hands-on training session, participating residents completed a structured questionnaire designed to evaluate their perceptions of the training program. The survey assessed four key domains: adequacy of trainee numbers, appropriateness of training duration, perceived procedural difficulty, and perceived usefulness of the training for future clinical practice. Responses were recorded using categorical options for each item.
Statistical analysis
Continuous variables from the DOPS evaluations were expressed as mean±standard deviation (SD). Differences in mean scores between cohorts were analyzed using the independent samples t-test; Welch’s t-test was applied when the assumption of equal variances was not met.
Categorical variables from the survey responses were summarized as frequencies and percentages, and differences in group distributions were assessed using the Pearson chi-square test or Fisher’s exact test, as appropriate.
All tests were two-sided, and a p<0.05 was considered statistically significant. Statistical analyses were performed using R software (version 4.4.2; R Foundation for Statistical Computing).
Results
Baseline characteristics and study flow
As detailed in the study flow diagram (Fig. 2), a total of 370 general surgery residents were initially enrolled in the standardized colonoscopy training program. Following the exclusion of one resident due to missing objective evaluation data, the final cohort for the DOPS analysis comprised 369 residents. This included 145 residents in the 2022 traditional cohort (target PGY-3) and 224 residents in the 2023–2025 early-intervention cohort (target PGY-2). For the subjective survey analysis, after excluding three non-respondents from the 2022 cohort and retaining two unidentifiable duplicate responses in the 2023–2025 cohort due to anonymous submission, a total of 369 responses (n=142 for the 2022 cohort; n=227 for the 2023–2025 cohort) were analyzed.
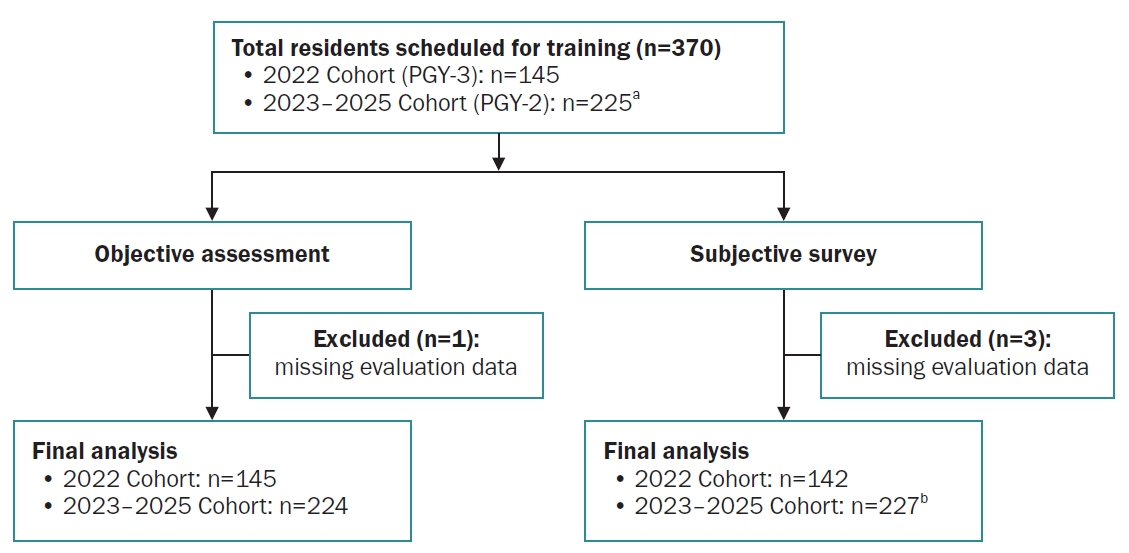
Flowchart of resident participation and analysis cohorts.
PGY, post-graduate year.
aIncludes 2 residents who completed training in PGY-3; bIncludes 2 unidentifiable duplicate responses.
Objective clinical competency (Direct Observation of Procedural Skills outcomes)
The results of the faculty-rated DOPS assessment are summarized in Table 2. Overall competency scores were high in both cohorts. There were no significant differences between PGY-3 and PGY-2 residents in Basic Manipulation Skills (10.74±1.37 vs. 10.60±1.55, p=0.380) or Anatomical Understanding and Documentation (5.63±0.70 vs. 5.54±0.81, p=0.214).
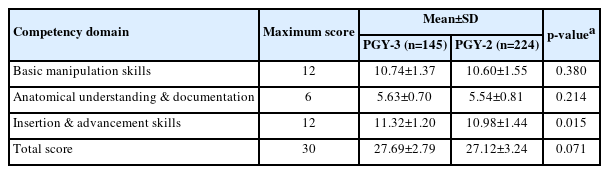
Comparison of domain-specific colonoscopy competency scores between PGY-3 and PGY-2 residents
In contrast, PGY-3 residents achieved significantly higher scores in Insertion and Advancement Skills compared with PGY-2 residents (11.32±1.20 vs. 10.98±1.44, p=0.015). The total DOPS score was slightly higher in PGY-3 residents but did not reach statistical significance (27.69±2.79 vs. 27.12±3.24, p=0.071).
Across all domains, mean scores exceeded 85% of the maximum possible score in both cohorts. To provide a more granular interpretation of procedural competency, item-level results corresponding to the assessment checklist are presented in Supplementary Table 2.
Trainee perceptions of the training program
Survey responses are summarized in Table 3. Most residents in both cohorts considered the number of trainees and the duration of the training session to be appropriate. Specifically, 96.5% of PGY-3 residents and 97.4% of PGY-2 residents reported that the trainee number was appropriate (p=0.551), while 85.9% and 85.5%, respectively, reported that the training time was appropriate (p=0.731).
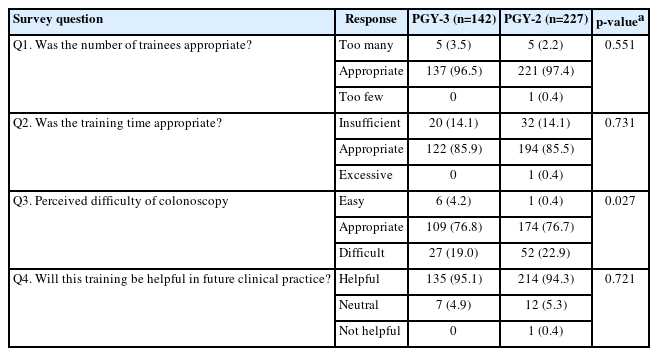
Trainee perceptions of the hands-on colonoscopy training program according to residency year
Regarding perceived procedural difficulty, the majority of participants rated the difficulty level as appropriate (76.8% in PGY-3 vs. 76.7% in PGY-2). However, PGY-2 residents more frequently reported the procedure as difficult compared with PGY-3 residents (22.9% vs. 19.0%), whereas PGY-3 residents more often rated the difficulty as easy (4.2% vs. 0.4%), resulting in a statistically significant difference between the groups (p=0.027).
Most residents reported that the training would be helpful for their future clinical practice (95.1% in PGY-3 vs. 94.3% in PGY-2, p=0.721).
Discussion
This study evaluated the outcomes of a standardized colonoscopy training program for general surgery residents using both objective competency assessment and trainee perceptions. Residents who participated in the training during their PGY-2 year achieved overall competency scores comparable to those of PGY-3 residents trained under the traditional model. However, domain-specific analysis revealed lower scores among PGY-2 residents in insertion and advancement skills. In addition, trainees from both cohorts reported high levels of acceptance of the training structure and perceived educational value. These findings provide insight into the early learning profile of surgical residents undergoing structured colonoscopy training.
The need for structured training in procedural education has been increasingly emphasized within competency-based medical education. Traditional apprenticeship-based training models rely heavily on variable clinical exposure and instructor-dependent teaching approaches, which may lead to inconsistencies in training experiences among residents [4,5]. In response, modern educational frameworks advocate clearly defined learning objectives, structured curricula, and objective workplace-based assessments to ensure consistent baseline competency [6-8]. Within endoscopy education, professional societies have similarly emphasized the importance of standardized training pathways and competency-based assessment systems to maintain procedural quality and patient safety [9,10].
The present training program was designed to address several of these educational considerations by integrating pre-learning modules, structured hands-on practice, and checklist-based competency assessment. The flipped-learning approach allowed residents to acquire foundational theoretical knowledge before attending the hands-on session, thereby enabling the practical training time to focus primarily on technical skill development. In addition, maintaining a low instructor-to-trainee ratio allowed individualized instruction and immediate feedback during procedural practice. Such educational strategies have been increasingly incorporated into procedural training programs in order to optimize learning efficiency within limited training time [18].
The domain-specific performance pattern observed in this study provides further insight into early colonoscopy skill acquisition. Residents in both cohorts demonstrated high scores in basic manipulation skills and anatomical recognition, suggesting that these competencies can be effectively introduced through structured training sessions. In contrast, lower scores were observed in insertion and advancement skills among PGY-2 residents. These procedural steps require integration of scope control, loop management, and spatial interpretation during navigation of complex colonic segments. Previous studies examining colonoscopy learning curves have consistently identified insertion and loop reduction as among the most technically demanding components of the procedure and among the last skills to be mastered by trainees [11-15,19]. The difference observed between PGY-2 and PGY-3 residents therefore likely reflects differences in cumulative procedural exposure rather than limitations of the standardized training program itself.
The high level of trainee acceptance observed in this study also supports the feasibility of implementing structured colonoscopy training early in surgical residency. Most residents reported that the number of trainees, the duration of the training session, and the overall educational format were appropriate, and the majority perceived the program to be beneficial for their future clinical practice. Evaluations of learner perceptions are commonly incorporated into educational research because they provide insight into the perceived effectiveness and practicality of training interventions within real educational environments [16,17].
Several limitations should be considered when interpreting the findings of this study. First, the study was conducted within a single structured training program, which may limit generalizability to other educational settings. Second, the evaluation focused on procedural performance immediately following the training session, and long-term skill retention or translation into clinical practice was not assessed. Third, although a structured checklist was used for objective competency assessment, formal inter-rater reliability among faculty evaluators was not evaluated. Finally, trainee perceptions were measured using self-reported survey responses, which may be influenced by response bias.
In conclusion, a standardized colonoscopy training program implemented early in surgical residency was associated with high levels of competency across most procedural domains. While overall competency was similar between PGY-2 and PGY-3 residents, insertion and advancement skills remained more challenging for earlier trainees. These findings suggest that early structured exposure may help establish foundational endoscopic skills, while continued clinical experience and targeted practice may be required for more advanced procedural tasks.
Supplementary Materials
Core technical components and DOPS-based assessment framework of the standardized colonoscopy training program
Item-level results of the assessment checklist for colonoscopy skills according to residency year
Notes
Disclosure
In-Seob Lee is and editor-in-chief and Sa-Hong Min is an associate editor of the journal, but they were not involved in the evaluation or decision-making process for this article and adhered to the decision made by independent reviewers. No other potential conflicts of interest relevant to this article was reported.
Acknowledgments
The authors gratefully acknowledge the Korean Surgical Society and the Korean Surgical Skill Study Group for their support in organizing and supporting this training program. We also thank the faculty instructors who actively participated in the hands-on training sessions and contributed to the education of surgical residents.
Author contributions
Conceptualization: DKS, SHJ, SJR, SHM, ISL; Supervision: DKS, SHJ, SHM, ISL; Writing–original draft: DKS, SJR; Writing–review & editing: DKS, SHJ, SJR, SHM, ISL.