Abstract
- Feeding jejunostomy is crucial for patients with compromised oral intake, particularly after gastrointestinal surgery or esophagectomy. Traditional methods involve interrupted sutures to secure the feeding tube to the abdominal wall, but this can be cumbersome due to the need for knot tying. This paper presents the case of a 75-year-old male patient who underwent minimally invasive esophagectomy with feeding jejunostomy for esophageal cancer, and introduces the use of a knotless barbed suture, which is commonly employed in gastrointestinal operations. The laparoscopic procedure utilized four trocars for jejunostomy, employing a 3-0 silk purse string suture and a 14-Fr Foley catheter. The barbed suture was used to secure the catheter in place without knots, covering 360° around the catheter. This method aims to simplify laparoscopic feeding jejunostomy and improve clinical practice.
-
Keywords: Laparoscopy, Jejunostomy, Suture technique
Introduction
Nutrition is supplemented with parenteral or enteral nutrition If oral feeding is impossible or insufficient [1]. Enteral nutrition methods include nasogastric, nasojejunal tube, gastrostomy, and jejunostomy. Among them, feeding jejunostomy has the advantage of reducing nausea and vomiting and lowering the risk of aspiration [2,3]. In particular, jejunostomy is widely used to improve the nutritional status of patients with expected complicated postoperative recovery after gastrointestinal surgery or esophagectomy, and severe dysphagia due to esophageal or pharyngeal malignancies [4,5].
Laparoscopic feeding jejunostomy is a generally accepted procedure with higher rate of success and lower rate of complications [6,7]. To prevent dislocation of the tube, interrupted sutures are performed to anchor the tube with an abdominal wall. The authors used a knotless barbed suture, which has been widely used in gastrointestinal surgeries, to more easily anchor the tube to the abdominal wall. We would like to briefly introduce our method of laparoscopic feeding jejunostomy using the barbed suture material, which is performed after esophagectomy.
Case Presentation
Patient
A 75-year-old male patient who had suffered dysphagia was diagnosed with an ulcero-infiltrative mass at between 28 and 34 cm from an upper incisor, occupying about half of the lumen. Chest computed tomography showed reactive lymph nodes in the subaortic area, subcarina, both hilar and interlobar areas, and both axillae. He was diagnosed as cT4N1M0 and underwent neoadjuvant concomitant chemotherapy (5-fluorouracil, cisplatin) and radiation therapy (45 GY, 5 weeks) three times. Afterwards, transthoracic esophagectomy and reconstruction were planned. In the selective patients, we are performing placement of feeding jejunostomy concomitantly. This study was approved by the Institutional Review Board (approval number: PC24ZASI0151). Informed consent from the patient was waived due to retrospective study design and anonymized data.
Surgical procedure
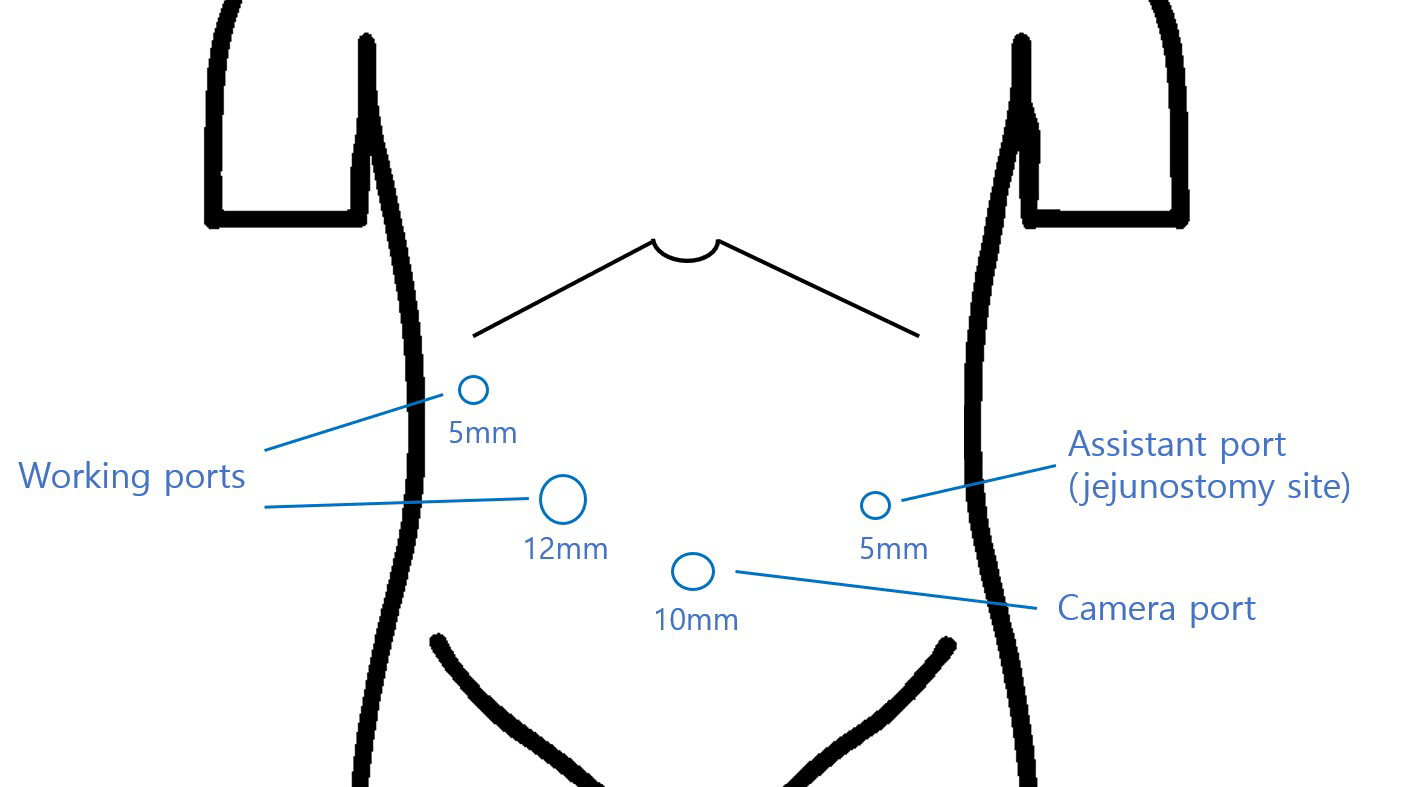
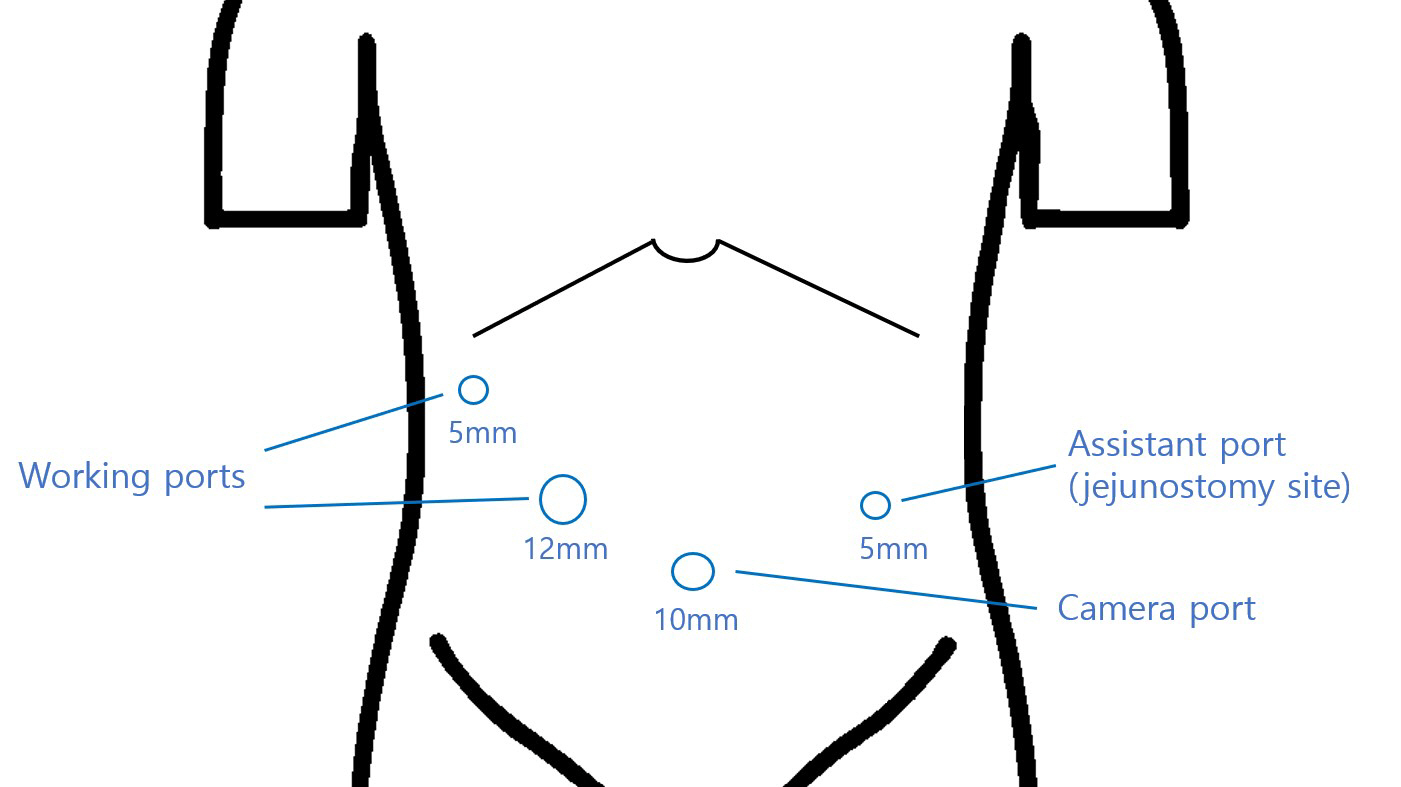
Surgical procedure video is edited and presented. After esophageal transection using a transthoracic approach, a gastric tube was created laparoscopically, and esophago-gastric anastomosis was made at the cervical level. Afterwards, jejunostomy was performed using the four trocars inserted during laparoscopic surgery (Fig. 1); a 5 mm port in the right upper quadrant and a 12 mm port between the umbilicus and the 5 mm port as the operator’s working ports, a 10 mm port at the umbilicus for the camera, and a 5 mm port at upper portion of left lower quadrant port for the assistant. When only feeding jejunostomy was performed, the port for the jejunostomy tube was inserted into the upper portion of left lower quadrant located between the mid-clavicular line and the anterior axillary line, and usually on the lateral side of rectus muscle, where the jejunal target insertion point is easily retractable to peritoneum. To fix jejunostomy catheter, intra-corporeal purse-string suture was performed using silk 3-0 thread on the proximal jejunum, approximately 20 cm away from a Treitz ligament. A small enterotomy was made using electrocautery inside the purse string suture. A 14-Fr foley catheter was inserted into the enterotomy via the left lower quadrant port site. The foley balloon was inflated with 3 mL of distilled water. The purse string suture was tied to secure the catheter so that it would not retract. To prevent torsion, alignment maintained so that the proximal jejunum was located at 2 o’clock and the distal was located at 8 o’clock, consistent with the anatomical location of the jejunum. One 3-0 absorbable knotless barbed continuous suture (Monofix) initiated at the peritoneum of the abdominal wall and seromuscular layer of the jejunum around the catheter. Importantly, initial suturing should begin at the jejunum and peritoneum where the view is obscured by the tube. In the same way, the purse string suture covering eight directions, and 360 degrees was performed. Afterward, the patency of the tube was checked, and fixed to the skin.
Discussion
Enteral nutrition is generally preferred to parenteral nutrition, as it is associated with fewer complications rates and enhanced recovery. Feeding jejunostomy is indicated in cases of gastric outlet obstruction and severe gastroparesis and can reduce nausea and vomiting after enteral feeding [1,8].
Due to recent advances in equipment and techniques of minimally invasive surgery, feeding jejunostomy is widely performed by laparoscopic method [7,9]. Anchoring the feeding jejunostomy to the abdominal wall is important; previously, it was necessary to suture between the abdominal wall and the jejunum using two or more interrupted sutures. However, interrupted suture through laparoscopy is somewhat troublesome because it requires tying knots. To improve this, we tried anchoring the feeding jejunostomy with one barbed suture, which is extensively used in gastrointestinal surgery. There is no significant difference compared to the existing interrupted suture during the feeding jejunostomy procedure, but the major advantage is that it can be easily fixed in eight directions without making knots.
In addition, our method has several features. In general, jejunostomy tube is preferred for feeding jejunostomy because it is not clogged and not easily damaged compared to silicone tubes [1]. However, the authors use the foley catheter because of being easily available, durable, and not subject to retraction due to the balloon. Witzel procedure of feeding jejunostomy is a surgical technique, placing a feeding tube into the jejunum and securing it with a seromuscular tunnel to minimize complications like spillage [10]. At our institution, laparoscopic feeding jejunostomies using barbed sutures were performed in 20 cases, and there were no complications such as spillage, dislocation, or kinking even without tunneling. Even after removal of the tube, tract was spontaneously closed without enteric fistula. It might be dependent on minimal skin incision, purse-string suture and tight enteric seromuscular to peritoneal approximation with barbed suture material. Additionally, while the mean operation time of Witzel method was 45 minutes [10], that of our method was less than 10 minutes. Therefore, our method is safe and efficient for laparoscopic feeding jejunostomy.
Fixation using barbed suture material is a technically simple and safe method when forming the feeding jejunostomy, and it is hoped that it will be used in actual clinical practice as well.
Disclosure
No potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization, Data curation, Formal analysis, Investigation: SHP, DJK; Methodology, Project administration: DJK; Resources: SHP, DJK; Supervision, Validation: DJK; Visualization: SHP; Writing–original draft: DJK; Writing–review & editing: SHP, DJK.
Figure 1.Placement of trocars for laparoscopic feeding jejunostomy. One 10-mm camera port was inserted at the umbilical level, as well as two working ports for the operator at the right upper quadrant (5 mm) and right lower quadrant (12 mm), respectively. Another 5-mm assistant port was placed at the upper portion of the left lower quadrant and was used for the jejunostomy site.
REFERENCES
- 1. Boullata JI, Carrera AL, Harvey L, Escuro AA, Hudson L, Mays A, et al. ASPEN safe practices for enteral nutrition therapy [formula: see text]. JPEN J Parenter Enteral Nutr. 2017;41:15-103.ArticlePubMed
- 2. ASGE Training Committee 2013-2014; Enestvedt BK, Jorgensen J, Sedlack RE, Coyle WJ, Obstein KL, et al. Endoscopic approaches to enteral feeding and nutrition core curriculum. Gastrointest Endosc. 2014;80:34-41.ArticlePubMed
- 3. Finucane TE, Bynum JP. Use of tube feeding to prevent aspiration pneumonia. Lancet. 1996;348:1421-1424.ArticlePubMed
- 4. Gabor S, Renner H, Matzi V, Ratzenhofer B, Lindenmann J, Sankin O, et al. Early enteral feeding compared with parenteral nutrition after oesophageal or oesophagogastric resection and reconstruction. Br J Nutr. 2005;93:509-513.ArticlePubMed
- 5. Wolthuis AM, Vanrijkel JP, Aelvoet C, De Weer F. Needle catheter jejunostomy complicated by pneumatosis intestinalis: a case report. Acta Chir Belg. 2003;103:631-632.ArticlePubMed
- 6. Hsiung T, Chao WP, Chai SW, Chou TC, Wang CY, Huang TS. Laparoscopic vs. open feeding jejunostomy: a systemic review and meta-analysis. Surg Endosc. 2023;37:2485-2495.ArticlePubMedPDF
- 7. Tsai HI, Chou TC, Yu MC, Yeh CN, Peng MT, Hsieh CH, et al. Purely laparoscopic feeding jejunostomy: a procedure which deserves more attention. BMC Surg. 2021;21:37.ArticlePubMedPMCPDF
- 8. Ukleja A, Sanchez-Fermin M. Gastric versus post-pyloric feeding: relationship to tolerance, pneumonia risk, and successful delivery of enteral nutrition. Curr Gastroenterol Rep. 2007;9:309-316.ArticlePubMedPDF
- 9. Bakhos C, Patel S, Petrov R, Abbas A. Jejunostomy-technique and controversies. J Vis Surg. 2019;5:33.ArticlePubMedPMC
- 10. Lotti M, Capponi MG, Ferrari D, Carrara G, Campanati L, Lucianetti A. Laparoscopic Witzel jejunostomy. J Minim Access Surg. 2021;17:127-130.ArticlePubMedPMC
Citations
Citations to this article as recorded by


 , Dong Jin Kim
, Dong Jin Kim
 PubReader
PubReader ePub Link
ePub Link Cite this Article
Cite this Article