
Articles
- Page Path
- HOME > J Surg Innov Educ > Volume 2(2); 2025 > Article
-
How I Do It
High Lymph Node Dissection with Low Ligation: A Modified Technique for Left Colic Artery Preservation in Colorectal Cancer -
Jesung Park1
 , Beom Gyu Kim1,2, Yong Gum Park1,2, Byung Kwan Park1,2
, Beom Gyu Kim1,2, Yong Gum Park1,2, Byung Kwan Park1,2 -
Journal of Surgical Innovation and Education 2025;2(2):27-30.
DOI: https://doi.org/10.69474/jsie.2025.00339
Published online: December 18, 2025
1Department of Surgery, Chung-Ang University Hospital, Seoul, Republic of Korea
2Department of Surgery, Chung-Ang University College of Medicine, Seoul, Republic of Korea
- Corresponding author: Byung Kwan Park, MD Department of Surgery, Chung-Ang University Hospital, 102 Heukseok-ro, Dongjak-gu, Seoul 06973, Republic of Korea Tel: +82-2-6299-1548, Fax: +82-2-6299-2017, E-mail: headlet@cau.ac.kr
© 2025 Korean Surgical Skill Study Group
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 43 Views
- 28 Download
Abstract
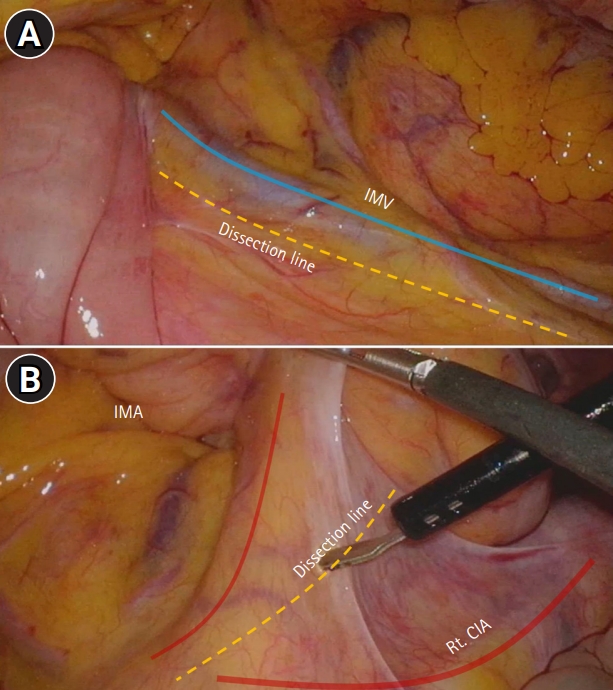
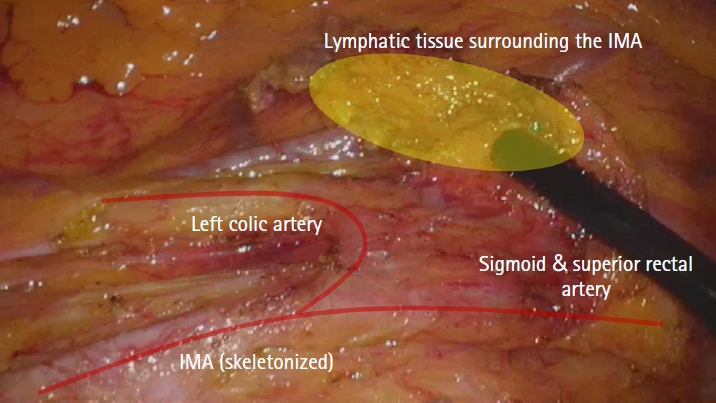
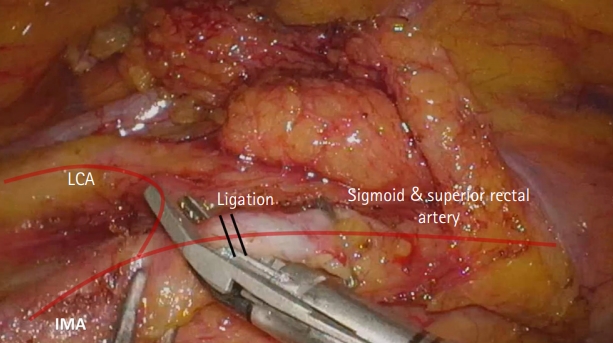
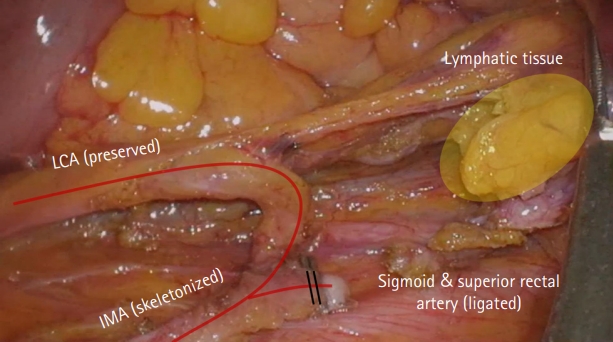
- The optimal level of inferior mesenteric artery (IMA) ligation in colorectal cancer remains controversial. High ligation allows complete D3 lymphadenectomy but sacrifices the left colic artery (LCA), raising concerns about anastomotic ischemia. This report presents a modified low ligation technique that achieves radical D3 dissection while preserving the LCA. The technique involves complete skeletonization of the IMA root with en bloc removal of surrounding lymphatic tissue while maintaining LCA continuity. Key procedural steps include: (1) medial-to-lateral mobilization, (2) exposure of the IMA origin, (3) para-IMA lymph node dissection along the vascular sheath, (4) preservation of the LCA and autonomic plexus, and (5) distal IMA division below the LCA bifurcation. Intraoperative images illustrate the dissected nodal field and preserved vasculature. This technique enables D3-level lymph node dissection comparable to high ligation, with clear visualization of the IMA root and preserved arterial supply. Thirty-five lymph nodes, including one metastatic node, were retrieved without compromising perfusion. This modified approach balances oncologic completeness with physiologic preservation and may serve as a practical model for achieving D3 lymphadenectomy with vascular preservation.
Introduction
Case Presentation
Discussion
Disclosure
No potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization: JP, BKP; Data curation: JP, BGK, YGP; Formal analysis: JP; Investigation: JP; Methodology: JP, BGK, YGP; Project administration: BKP; Software: JP; Supervision: BKP; Validation: BGK, YGP; Visualization: JP; Writing–original draft: JP; Writing–review & editing: BGK, YGP, BKP.
- 1. Kim K, An S, Kim MH, Jung JH, Kim Y. High versus low ligation of the inferior mesenteric artery in colorectal cancer surgery: a systematic review and meta-analysis. Medicina (Kaunas). 2022;58:1143.ArticlePubMedPMC
- 2. Zeng J, Su G. High ligation of the inferior mesenteric artery during sigmoid colon and rectal cancer surgery increases the risk of anastomotic leakage: a meta-analysis. World J Surg Oncol. 2018;16:157.ArticlePubMedPMCPDF
- 3. Pigazzi A, Ellenhorn JD, Ballantyne GH, Paz IB. Robotic-assisted laparoscopic low anterior resection with total mesorectal excision for rectal cancer. Surg Endosc. 2006;20:1521-1525.ArticlePubMedPDF
- 4. Akagi T, Inomata M, Hara T, Mizusawa J, Katayama H, Shida D, et al. Clinical impact of D3 lymph node dissection with left colic artery (LCA) preservation compared to D3 without LCA preservation: exploratory subgroup analysis of data from JCOG0404. Ann Gastroenterol Surg. 2020;4:163-169.ArticlePubMedPMCPDF
- 5. West NP, Hohenberger W, Weber K, Perrakis A, Finan PJ, Quirke P. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol. 2010;28:272-278.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

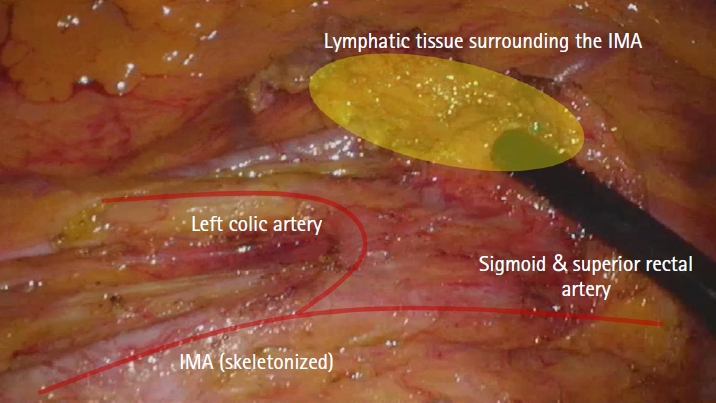
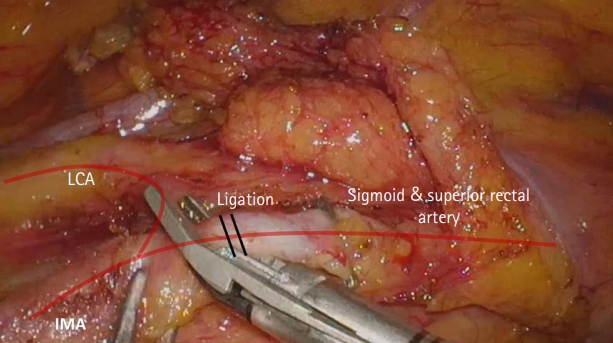
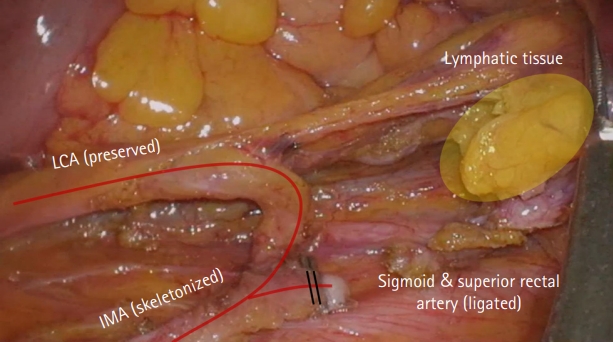




Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
TOP

