Techniques in Jejunojejunostomy, Gastrojejunostomy, and Esophagojejunostomy in Reduced-Port Gastrectomy
Article information

Abstract
Minimally invasive gastric cancer surgery aims to reduce morbidity and mortality while maintaining satisfactory oncological outcomes. Laparoscopic gastrectomy is a standard treatment, offering reduced pain, shorter hospital stays, and faster recovery. Reduced-port gastrectomy has gained popularity due to its requirement for limited assistants; however, it poses unique challenges. This paper shares the techniques used in three cases of jejunojejunostomy, gastrojejunostomy, and esophagojejunostomy during reduced-port gastrectomy. Reduced-port techniques were successfully implemented in all three cases. Key steps included proper port placement, the use of tagging sutures, and strategic stapler insertion and adjustment. The reduced-port approach demonstrated feasibility and effectiveness despite its inherent challenges. Reduced-port gastrectomy can be effectively performed with a careful technique and meticulous planning, despite the challenges of transitioning from conventional five-port techniques. Using fewer ports results in less pain, fewer complications, and shorter hospital stays without compromising oncologic outcomes. These techniques can be helpful for trainees and novice surgeons, though careful candidate selection is paramount.
Introduction
Minimally invasive gastric cancer surgery, encompassing both laparoscopic and robotic approaches, aims to reduce morbidity and mortality while maintaining or enhancing oncological outcomes [1]. Currently, laparoscopic gastrectomy is regarded as one of the standard treatments for gastric cancer, offering benefits such as reduced pain, shorter hospital stays, and faster recovery [2]. Reduced port gastrectomy has recently gained popularity among young surgeons in several institutions, primarily due to limited availability of assistants, making it a challenging procedure. Among the many types of anastomoses involved in gastric cancer surgery, this paper aims to share my technique for performing jejunojejunostomy, gastrojejunostomy, and esophagojejunostomy during reduced port gastrectomy.
Case Presentation
The three cases introduced in this paper were all performed using reduced port gastrectomy. Fig. 1 shows the port placements of the three cases. To emphasize the techniques used in anastomoses, all descriptions of the gastrectomy procedure itself have been omitted.
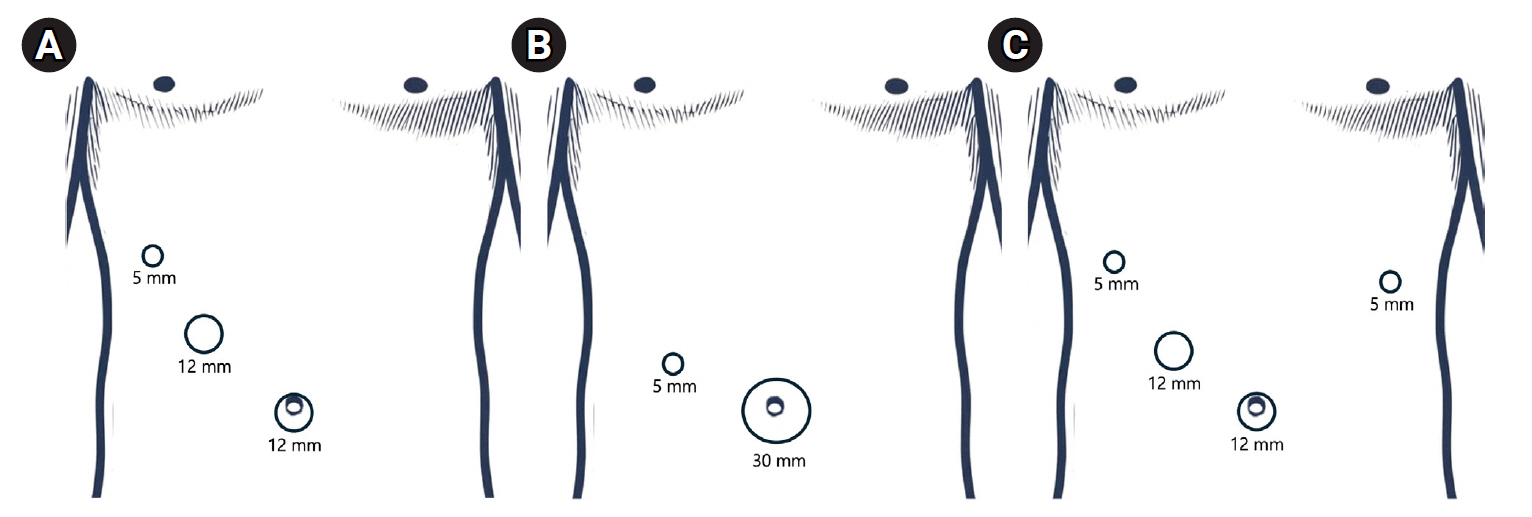
Laparoscopic port placements for the three cases. (A) Three-port surgery, (B) 2-port surgery, (C) 4-port surgery.
Jejunojejunostomy with three ports and no assistant
Three ports were used for this surgery (Fig. 1A): a 5 mm port in the right upper quadrant (RUQ) and a 12 mm port between the umbilicus and the 5 mm port as the operator’s working ports, and a 12 mm port at the umbilicus for the camera (as depicted in the video). When creating both entry holes, the electrocautery device was used almost perpendicular to the jejunal wall to avoid surrounding tissue damage and to facilitate easier widening of the hole. Inserting the surgical stapler into the entry holes can be challenging for novice surgeons without an assistant. The key point is to ensure the tip of the cartridge side of the stapler is placed in the entry hole and to apply counter traction to the jejunum, similar to pulling on socks. After inserting the anvil side of the stapler, slipped jejunum is pulled for adjustments and the surgical stapler is fired. Avoid pulling the jejunum too hard while inserting both tips of the surgical stapler. Excessive tension can result in a large common entry hole, which can affect the anastomosis size after closure. The first tagging suture is placed on the far end of the common entry hole and tied using a knot pusher. Subsequently, the second tagging suture is placed at the nearer end, which is then pulled from the outside by the scrub nurse instead of being cut. The last tagging suture is placed in the middle to close the common entry hole and to prevent the tissue from sagging or spreading apart. When inserting the stapler, it should always be positioned under the pulled tagging suture so that it acts as an assistant. Ensure that both sides of the jejunal wall are positioned between the stapler, just above or at the same level as the upper border of the stapler, to ensure maximum anastomosis size. Applying pressure on the tissue by closing the stapler once or twice can provide a better view for minimal stapling. The overlapping area of the stapler lines can be vulnerable to ischemia, so a reinforcement suture at this site can provide additional security.

Gastrojejunostomy with two ports and no assistant
Two ports were used for this surgery (Fig. 1B): a 3 cm single incision at the umbilicus using a multichannel port, and one additional 5 mm port positioned 8 cm from the umbilical port towards the RUQ. When making an entry hole in the remnant stomach, it is easier to do so at the distal end of the stapler line along the greater curvature, which also facilitates closing the common entry hole with minimal narrowing of the anastomosis. After puncturing, suctioning the inside of the stomach is crucial to avoid any spillage of gastric contents when performing the anastomosis, which is different from making the entry hole in the small bowel. Inserting the stapler into the entry holes can be even more challenging when it is inserted from the umbilicus direction. Press the tip of the cartridge side of the stapler to the entry hole, and perform a sock-pulling motion. After fully inserting the anvil side, the stomach and the jejunum are then pulled for adjustments before firing the stapler. As described in the jejunojejunostomy section above, tagging sutures and closure of the common entry hole are performed in the same manner, with the bottom suture being pulled from the outside through the multichannel port for traction.
Esophagojejunostomy with four ports and one assistant arm
Four ports were used for this surgery (Fig. 1C): two 5 mm ports in the RUQ and the left upper quadrant (LUQ), and two 12 mm ports, one at the umbilicus for the camera and one between the umbilicus and the RUQ port. The esophagus is cut at the marked spot with a stapler, leaving one-third of the esophagus. This helps to identify the true lumen and prevents the operator from inserting the stapler into a false lumen. After insertion of the cartridge side of the stapler into the jejunum, it is pulled alongside the remnant esophagus. The anvil side is then inserted into the true lumen of the esophagus and closed. Since the esophagus tends to be pulled into the mediastinum, the operator must pull the esophagus during the anastomosis. The assistant’s one arm is required to pull the slipped jejunum for adjustments before firing the stapler. Closure of the common entry hole can be done identically to the procedures described for jejunojejunostomy or gastrojejunostomy.
Discussion
Reduced number of ports makes the entire surgery challenging due to the accustomed training with conventional five-port techniques. Additionally, the centralization of surgeons and surgical residents has led to many hospitals suffering from a lack of assistants. Fortunately, according to several studies, using fewer ports can result in less pain, fewer complications, and shorter hospital stays, with no difference in oncologic outcomes [3-7]. For trainees and novice surgeons, the techniques demonstrated in this paper may be helpful but are just one of many possible techniques, and modifications can be made according to the surgeon’s preference. It is essential to carefully select the best candidates for these procedures.
Notes
Disclosure
Sa-Hong Min is an associate editor of the journal, but he was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.