
Articles
- Page Path
- HOME > J Surg Innov Educ > Volume 2(1); 2025 > Article
-
How I Do It
How to Perform Single-Incision Laparoscopic Totally Extraperitoneal Hernia Repair -
Moon Jin Kim
 , Ji Hoon Kim, Ju Myung Song, Chae Dong Lim
, Ji Hoon Kim, Ju Myung Song, Chae Dong Lim -
Journal of Surgical Innovation and Education 2025;2(1):14-18.
DOI: https://doi.org/10.69474/jsie.2025.00059
Published online: June 26, 2025
Department of Surgery, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
- Corresponding author: Ji Hoon Kim, MD, PhD Department of Surgery, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 56 Dongsoo-ro, Bupyeong-gu, Incheon 21431, Republic of Korea Tel: +82-32-280-5024, Fax: +82-32-280-5556, E-mail: samryong@catholic.ac.kr
• Received: May 8, 2025 • Revised: June 9, 2025 • Accepted: June 17, 2025
© 2025 Korean Surgical Skill Study Group
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 43 Views
- 32 Download
Abstract
- Surgery for inguinal hernia has made significant progress over a period of more than a century. The advent of minimally invasive techniques prompted further innovations. Among these, single-incision surgery offers significant advantages in creating the preperitoneal space. Therefore, it is essential for surgeons to understand and be able to perform single-incision laparoscopic totally extraperitoneal (SIL-TEP) hernia repair. This article presents a detailed description of the surgical technique for SIL-TEP.
Introduction
Case Presentation
Skin incision
Fundamental technique of single-incision laparoscopic surgery
Intraperitoneal procedure (video)
(1) Step 1. Space making (preperitoneal space dissection)
(2) Step 2. Identify the anatomy and hernia
(3) Step 3. Handling of hernia sac
(4) Step 4. Parietalization
(5) Step 5. Placement of the mesh
Discussion
Disclosure
No potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization: MJK, JHK, JMS, CDL; Supervision: MJK, JMS; Writing–original draft: MJK; Writing–review & editing: MJK, JHK, JMS, CDL.
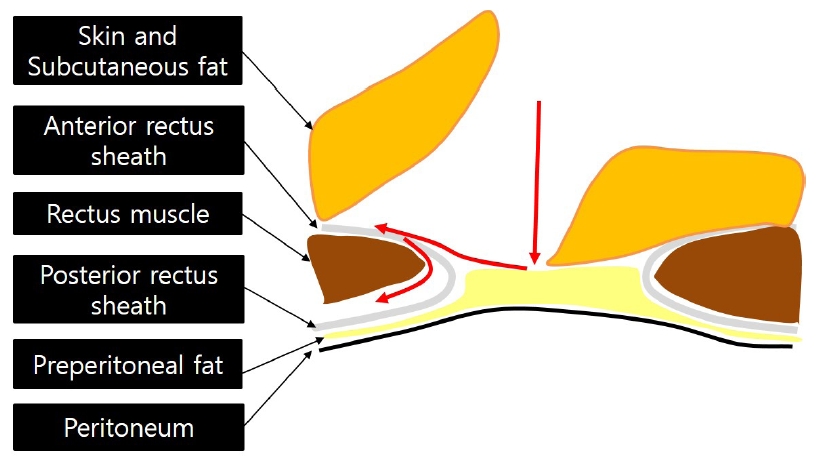
Fig. 1.Diagram illustrating the approach to the retro-rectus space via a trans-umbilical skin incision. The red arrowline indicates the direction of surgical progression.
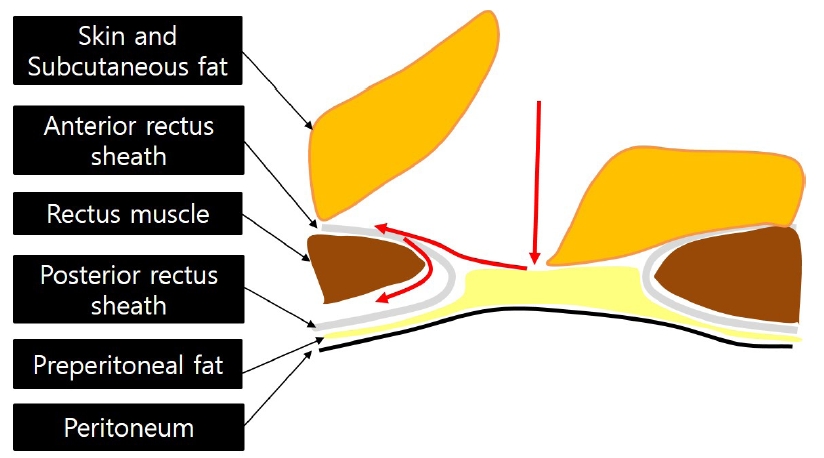
Fig. 2.(A) Proper positioning of the scope and the two instruments. (B) Improper instrument alignment. (C) Schematic illustration of instrument positioning based on the target anatomy.

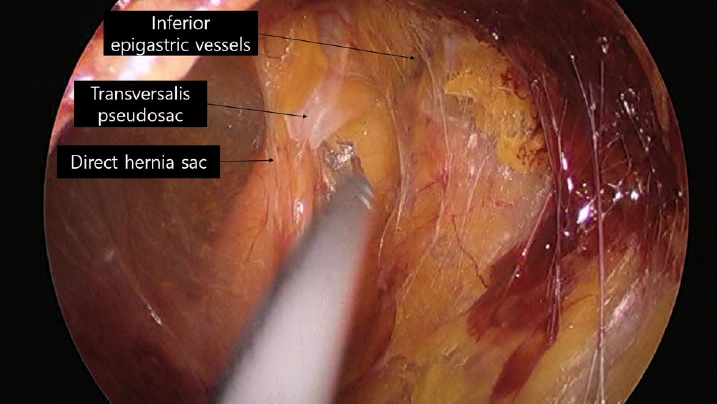
Fig. 3.Surgical view of a direct hernia. The outer layer of the hernia sac consists of preperitoneal tissue.
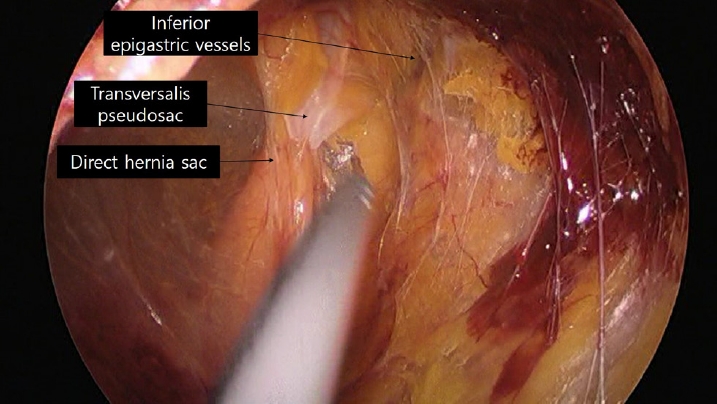
Fig. 4.(A) Appearance after reducing the direct hernia sac. A hernia defect is observed within Hesselbach’s triangle on the medial side of the inferior epigastric vessels. (B) The transversalis pseudosac is pulled. (C) The pseudosac is fixed to Cooper’s ligament using a tack.

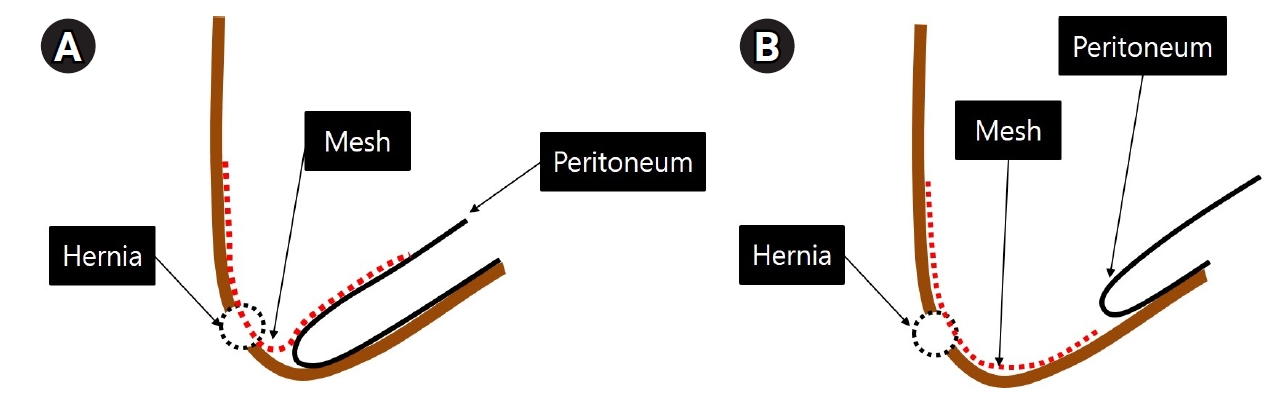
Fig. 5.(A) Insufficient parietalization results in mesh folding after surgery. (B) Adequate parietalization ensures the peritoneum naturally covers the mesh without folding.
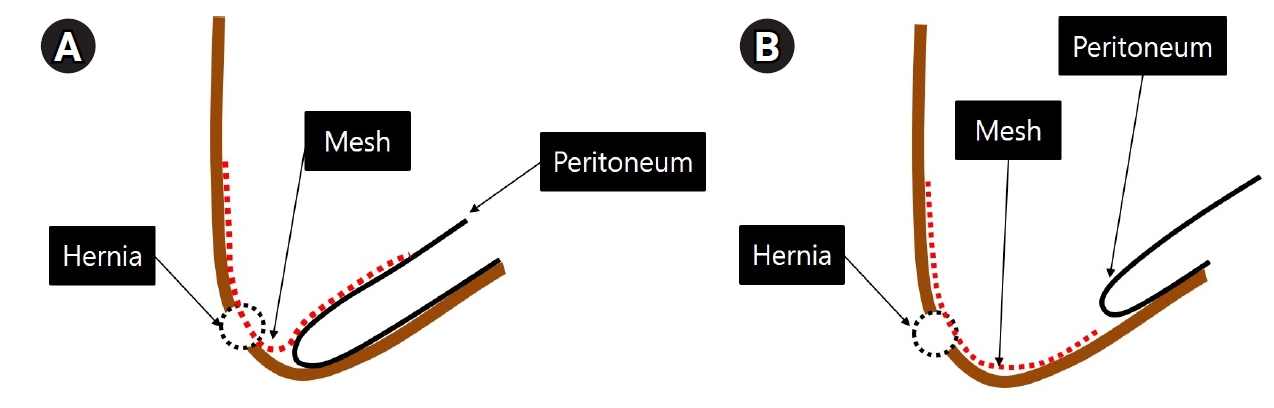
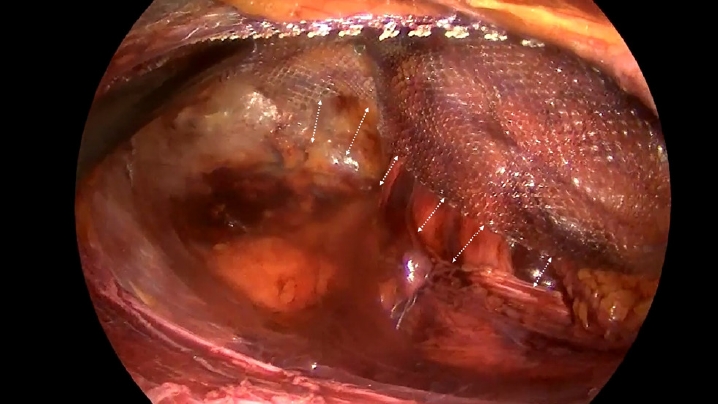
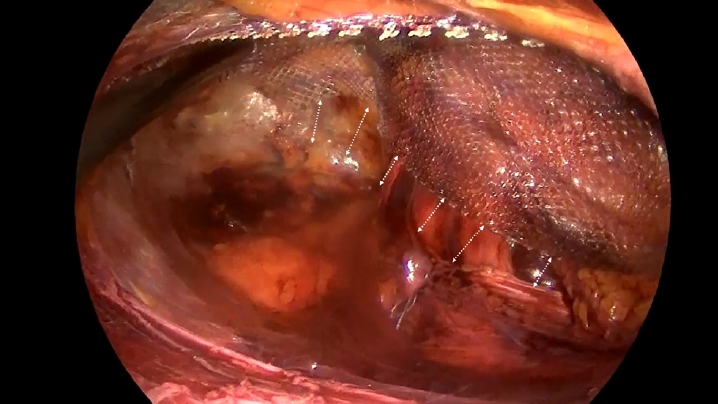
Fig. 6.Maintaining an appropriate distance between the mesh and peritoneal reflection prevents mesh folding after gas removal from the surgical space.
- 1. Lichtenstein IL, Shulman AG, Amid PK, Montllor MM. The tension-free hernioplasty. Am J Surg. 1989;157:188-193.ArticlePubMed
- 2. Corbitt JD Jr. Laparoscopic herniorrhaphy. Surg Laparosc Endosc. 1991;1:23-25.ArticlePubMedPDF
- 3. Perivoliotis K, Tzovaras G, Sarakatsianou C, Baloyiannis I. Current status of single-port versus multi-port approach in laparoscopic inguinal hernia mesh repair: an up-to-date systematic review and meta-analysis. Hernia. 2019;23:217-233.ArticlePubMedPDF
- 4. Kim JH, An CH, Lee YS, Kim HY, Lee JI. Single incision laparoscopic totally extraperitoneal hernioplasty (SIL-TEP): experience of 512 procedures. Hernia. 2015;19:417-422.ArticlePubMedPDF
- 5. Lee YJ, Kim JH, Kim CH, Lee GR, Lee YS, Kim HJ. Single incision laparoscopic totally extraperitoneal hernioplasty: lessons learned from 1,231 procedures. Ann Surg Treat Res. 2021;100:47-53.ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-


How to Perform Single-Incision Laparoscopic Totally Extraperitoneal Hernia Repair






Fig. 1. Diagram illustrating the approach to the retro-rectus space via a trans-umbilical skin incision. The red arrowline indicates the direction of surgical progression.
Fig. 2. (A) Proper positioning of the scope and the two instruments. (B) Improper instrument alignment. (C) Schematic illustration of instrument positioning based on the target anatomy.
Fig. 3. Surgical view of a direct hernia. The outer layer of the hernia sac consists of preperitoneal tissue.
Fig. 4. (A) Appearance after reducing the direct hernia sac. A hernia defect is observed within Hesselbach’s triangle on the medial side of the inferior epigastric vessels. (B) The transversalis pseudosac is pulled. (C) The pseudosac is fixed to Cooper’s ligament using a tack.
Fig. 5. (A) Insufficient parietalization results in mesh folding after surgery. (B) Adequate parietalization ensures the peritoneum naturally covers the mesh without folding.
Fig. 6. Maintaining an appropriate distance between the mesh and peritoneal reflection prevents mesh folding after gas removal from the surgical space.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
How to Perform Single-Incision Laparoscopic Totally Extraperitoneal Hernia Repair
TOP

